Hypothermia
AUTHOR: DR LUCY LONGBOTTOM
Cold injury is a serious danger at high altitude, particularly in winter seasons but with appropriate training, can be quickly recognised and managed or prevented with adequate preparation. Pathologically, cold injury can be divided into accidental hypothermia and localised non-freezing injuries or frostbite; we will focus on accidental hypothermia which refers to an involuntary drop in core body temperature below 35°C, a potentially fatal condition. Accidental is used to distinguish it from induced or therapeutic hypothermia (1).
Pathophysiology of hypothermia
Thermoregulation is a homeostatic mechanism within the body, under hypothalamic control, that strives to maintain constant internal conditions, regardless of external factors such as environmental temperature. Peripheral temperature receptors send signals to the hypothalamus which relays signals via the sympathetic nervous system to the brain stem to initiate responses such as shivering (involuntary thermogenesis), and peripherally to pilo-erector muscles, peripheral vasculature and sweat glands. In cold environments, the body uses negative feedback to attempt to prevent further heat loss in the form of peripheral vasoconstriction and redistribution of blood centrally, and shivering to generate further heat production.2 In mild environments, core body temperature can be maintained by behavioural responses i.e. wearing more layers, finding shelter and exercising (voluntary non-shivering thermogenesis).
What are causes of hypothermia
Accidental hypothermia develops when one or more of the following principles occur:
- Decreased heat production: e.g. hypoglycaemia, dehydration, exhaustion, age, hypothyroidism, lack of adaptation
- Increased heat loss: e.g. immersion/exposure to cold, alcohol, burns, heatstroke
- Impaired thermoregulation: e.g. trauma, drug & alcohol, TBI (traumatic brain injury), hypothyroidism, hypovolaemia, low BMI, children (high SA(surface area):vol) (2)
Further factors can be present which will increase the risk of an individual to become cold:
- Mental state – fear and low mood
- Physiological condition – unwell, slim individuals, physical fitness
- Team morale – lack of group communication and encouraging morale
- Nutrition – lack of energy, lack of warm food to warm person from inside
- Kit & equipment – poor quality, not enough layers
Symptoms typically present at temperatures <35°C and develop insidiously over several hours, however the onset can be rapid if the body is immersed into cold water or snow. Thus, on expeditions we refer to two hypothermic categories:
- Exposure hypothermia: insidious onset over several hours following exposure to cold environment. Casualty often becomes exhausted as their energy reserves are depleted and they are no longer able to shiver and re-warm themselves.
- Immersion hypothermia: rapid onset following sudden immersion in cold water or snow (3)
When exposed to cold, heat can be lost from the body through 5 mechanisms:
- Radiation: Body heat transferred to another surface nearby such as cold rocks without touching them but instead via photons independent of the temperature of the intervening air. Most heat is lost in this manner.
- Convection: Heat is lost when a temperature gradient exists between internal and ambient temperature. Movement of air due to wind prevents the buildup of heat near the skin surface by displacing warm air with cooler air. Wind chill increases the speed of heat loss through convection and can thus lead to greatly reduced relative temperatures.
- Evaporation: Heat is lost when moisture dissipates into the surrounding air, taking heat with it e.g. perspiration when exercising and carrying a pack or wet skin or clothing.
- Conduction: Body heat is lost to rocks and cold ground through direct physical touch
- Respiration: Heat is lost when respiring, respiration rate increases when walking up at high altitude, thus increasing rate of heat loss
When mobility and conscious level are compromised, the core body temperature could drop at a significant rate. This depends on clothing, physiological factors, such as blood glucose and fatigue, and environmental factors, such as the temperature gradient between body and surrounding environment, wind and wet conditions. Cooling rates have been shown to vary from <1°C to 9.4°C per hour when temperature was measured continuously in simulated scenarios (1-3).
Physiological effects of cold
Cardiovascular:
Within the heart, the electrical system cools down faster than the myocardium, and as this occurs the heart rate slows, leading to bradycardia. As it cools, the myocardium becomes progressively more unstable leading to arrhythmias. As long as the heart is still beating the casualty can tolerate these arrhythmias, however, any sudden movements or further cooling of the myocardium will put the heart at high risk of going into ventricular fibrillation. Thus, caution must be exercised when managing and handling hypothermic casualties, particularly when trying to evacuate them. At temperatures less than 28°C the heart rate will slow considerably culminating in extreme bradycardia and subsequent asystole (4).
Peripheral vasoconstriction and thermogenesis are important mechanisms that occur almost immediately in response to heat losses. Cutaneous vasoconstriction minimises peripheral blood flow, thus reducing the flow of convective heat loss to the surrounding environment. However, this can be at detriment to a loss of dexterity which can increase further risks for the individual in managing their condition. Consequently, blood flow is redirected and the volume of blood circulating in the central system increases. As more blood flows through the renal system, the kidneys initiate cold diuresis which culminates in the excretion of warm urine and thus loss of warm blood (aka the internal hot water bottle!). Diuresis can predispose the casualty to hypovolaemia during rewarming when the peripheral circulation opens up again leading to the ‘afterdrop’ phenomenon which will be discussed later (2-4).
Trauma in a cold environment can be catastrophic as cold negatively impacts coagulation thus increasing the risk of further blood loss and subsequent hypovolaemia. At 33°C coagulation is thought to be reduced by 50%. Coagulopathy can also lead to an increase in lactic acidosis thus lowering the pH of the blood which can negatively impact cardiac function. Subsequent hypovolaemia and reduced cardiac output will increase the risk of hypothermia and further cooling. This cascade of events is often referred to using the “trauma triad of death” (5) as shown in figure 1.
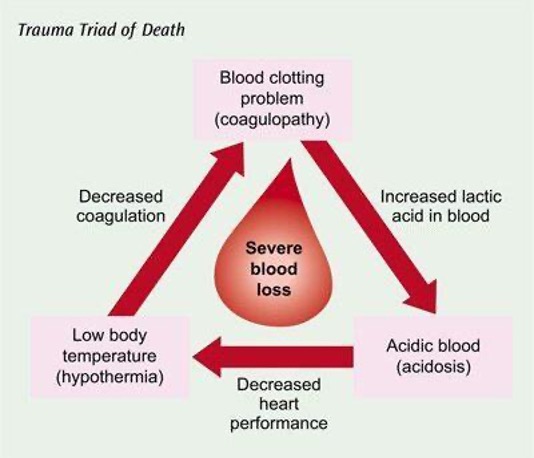
Figure 1: Trauma triad of death
Taken from: persysmedical.com
Neurological:
Neurological electrical impulses slow significantly in the cold and we call this the “umbles” phenomenon:
- Mumbles: dysarthria, confusion, sleepiness,
- Stumbles: ataxia, stiffness in extremities, reduced control and coordination
- Grumbles: apathy, altered behaviour,
- Fumbles: slow reaction time, reduced dexterity, poor coordination, dropping things
These symptoms can lead to dangers for both the casualty and the group as they become less physically and mentally capable to perform simple tasks. At temperatures less than 33°C brain electrical activity becomes abnormal. As the medic of the group, you must also remember that you are at risk of these dangers too and must protect yourself from further cooling as well as your group.
Metabolic:
Thermogenesis refers to heat production by voluntary behavioural (exercising) or involuntary(shivering) response mechanisms. Metabolic heat production during physical exercise can be significant as almost 70% of energy expended during muscle contraction is expelled as heat production. Shivering effectively increases heat generation by 6 times more than the basal metabolic rate. However, this also increases energy consumption at a cost of 5 times that of the resting metabolic rate (6) Thus, fatigue can limit the body’s ability to generate heat through thermogenesis. It is therefore unlikely for severe hypothermia to occur in a healthy responsive person who still has the ability to move. Although body habitus can affect this, those with an enlarged body habitus are considered to be better insulated by subcutaneous fat, whereas others are predisposed to accidental hypothermia and must rely on shivering and behavioural insulation using clothing and shelter (7).
Furthermore, insulin has a reduced efficiency in cold environments thus it is important to maintain a high level of awareness of any individuals with a diagnosis of diabetes as they can be at an increased risk of hyperglycaemic events. There is currently little research on the effects of other hormones in cold environments (8).
In a similar vein, the cold affects the efficiency of medications as drug metabolism slows. For example, when following the ALS algorithm for a hypothermic cardiac arrest, you are advised to allow double the time between administration of adrenaline doses in comparison to a normothermic casualty.
Presentation
Symptoms progress relative to the drop in core body temperature. Due to this, hypothermia can be classified in stages based upon physiological response and subsequent presenting symptoms:
| Core Temperature | Physiology | Presentation |
|---|---|---|
| Pre-hypothermia (>35°C) | Shivering | Consciously cold |
| Tachycardia | Shivering | |
| Peripheral vasoconstriction | ||
| Mild Hypothermia (33-34°C) | Cold diuresis | Ataxia |
| Progressive bradycardia | Worsening coordination | |
| Reduced cerebral metabolism | Reduced mental state | |
| Shallow breathing | Dysarthria | |
| Apathy | ||
| Moderate hypothermia (30-32°C) | Polkiothermic | Paradoxical undressing |
| Unable to shiver | Reduced consciousness | |
| Oxygen consumption decreases | Possible deterioration to coma | |
| Severe hypothermia (28°C) | Acid-base disturbance | |
| Reduced cerebral flow ~30% | ||
| 20°C | HR 20% of normal | |
| 18°C | Asystole |
The polikilothermic line occurs between 30-32°C and refers to the point at which the casualty is no longer able to rewarm themselves e.g. unable to initiate further shivering, and thus will need to be managed with active rewarming (1,3, 9).
The Swiss model (figure 2) is considered the internationally accepted staging criteria for hypothermia and its use has been advocated to estimate actual body temperature due to the symptoms the casualty is displaying. This then impacts on patient treatment and management without the need for a working thermometer. However it is important to recognise that each casualty is individual and their physiological response to exposure to the cold environment may differ slightly to the arbitrary temperature readings in the model (10).
| Stage | Clinical Symptoms | Typical Core Temp (°C) |
|---|---|---|
| Hypothermia I | Conscious | 35-32 |
| Shivering | ||
| Hypothermia II | Impaired consciousness | 32-28 |
| No shivering | ||
| Hypothermia III | Unconscious | 28-24 |
| No shivering | ||
| Vital signs present | ||
| Hypothermia IV | No or minimal vital signs | <24 |
Figure 2: The Swiss model of the staging and classification of hypothermia
Using the Swiss staging one can often assess a casualty’s degree of hypothermia base upon their presenting symptoms and physiological observations (9-12).
It is frequently difficult to get an accurate measurement of a casualty’s true core temperature in the remote setting. Core temperature is most accurately measured in the pulmonary artery however, it is difficult to access invasive thermometers in the field. Rectal, axilla and tympanic membranes can be used on expedition but it can take up to an hour for rectal temperatures to adjust for changes in core temperature and measurements from tympanic membrane and axillae are even less accurate.
In the field, we must also consider the ‘After drop’ phenomenon:
During rewarming, warm blood is drawn from the central body and then travels through the cold peripheral circulation. As it does so, the blood loses heat to the surrounding peripheral tissues and returns to the heart much colder than when it left through the aorta. This then cools the core body temperature further than before rewarming began and is thus termed “afterdrop.” As rewarming is already underway, casualties may begin to feel warmer at this time as their peripheries are perfused and subsequently start to remove layers which can lead to a further drop in the core body temperature. To this extent, after drop can lead to sudden clinical deterioration and subsequent death (1).
Hypothermia : how to manage the cold casualty
Management of a hypothermic casualty in the field revolves around the prevention of further heat loss and initiation of active rewarming. The extent to which you can initiate rewarming will be dependent on the kit that is available to you. Firstly, you must ensure that as the rescuer or medic, you must protect yourself from further cooling. Cooling causes ataxia and loss of fine motor control which you can’t afford to lose when caring for a hypothermic team member. Mental capacity, especially short term memory, decreases so we would advise taking an aide memoire with you on expedition and encouraging another team member to scribe so that there is a comprehensive record of information to handover to any emergency services should you require casualty evacuation. One must also consider the impact of the cold environment on your medical kit – many medications are prone to freezing , stuffing these inside your underwear can keep them from freezing! Or is there an alternative product you could take? (Questions to ask before you leave as frozen meds are heavy and useless!)
There are several methods of rewarming but they all boil down to 3 principles; passive external rewarming, active external rewarming and active internal rewarming (11-12). Treatment will be dependent on the degree of hypothermia that the casualty is experiencing. However, the initial management steps will remain the same for all casualties. Firstly, remove any wet clothing and replace this with dry clothing and insulation as soon as possible to prevent further deterioration.
A hypothermic ‘burrito’ wrap can be used for any degree of hypothermia to provide external insulation and prevent further heat loss through convection, conduction, radiation and evaporation. A hypothermic wrap has several layers; firstly, as the most external layer, a tarp is used to provide external protection from the environmental elements. A roll mat then provides insulation between the casualty and the wet or cold ground thus reducing heat loss via conduction. An aluminium foil blanket provides a layer of insulation by reflecting heat back towards the person inside the wrap and acting as a layer to avoid the casualty getting wet due to evaporation. Finally a sleeping bag is used to provide the innermost layers of insulation within which the casualty lies wearing dry clothes and any insulated jackets or layers available to them. A hat is used to cover the casualties head to prevent further heat loss as a large proportion of heat can be lost from the head due to its surface area. The layers of the wrap can be prepared in advance and rolled up together then strapped on the back of someone’s pack or even stuffed into the boat as a backrest on a kayak expedition – anywhere where it will be easily accessible! A demonstration of a hypothermic wrap is shown in the pictures below.

Figure 3: demonstration of a hypothermic wrap from a session on hypothermia during our Expedicine Medicine and Leadership Summer course
Mild hypothermia can be treated with passive external rewarming. Insulation is placed on the casualty to minimise further heat loss and retain any heat produced in shivering thermogenesis. It is recommended to aim to warm them by 0.5 to 2°C per hour. Equipment such as bivvi bag and storm shelter can be used to protect the casualty, and the rest of the team from the surrounding environment. Warm sweet drinks can further improve rewarming in conscious mild hypothermic casualties and can help to replace energy lost through shivering.
Moderate hypothermia will require passive and active external rewarming with minimal movement of the casualty where possible to reduce the risk of cardiac arrhythmias. Heat pad or water bottles filled with hot water can be used to warm central areas of increased blood flow such as the groin, axillae, and lateral bases of the neck. If bailable, blizzard blankets can be used for a combination of passive and active external rewarming with heat bands inserted inside the blanket. Sleeping bags can also be used but consideration must be taken over the type of material. Down provides effective insulation but only when pre-warmed (ask another warmer member of the team to wear it first and exercise in e.g. push ups to warm the down before allowing the cold casualty to wear it).
Severe hypothermia may require more invasive treatment involving active internal rewarming methods ranging from humidified air to cardiopulmonary bypass and extracorporeal membrane oxygenation (ECMO). Evacuation to definitive care will be required for intraperitoneal or intra pleural fluid rewarming before consideration for ECMO. Knowledge of the nearest ECMO can be crucial information at this stage and is worth investigating prior to starting the expedition.
As with casualties deemed to be suffering from moderate hypothermia, extra care should be taken with casualties with severe hypothermia and those with reduced consciousness to not move them if possible due to progressive cardiac instability and any jostle may precipitate a cardiac arrest. If casualty is in cardiac arrest then consider starting CPR. This is a much debated decision and is one that we would advise you to discuss with reach back or top cover if possible. Mountain Rescue England & Wales have produced really useful guidelines on when to start CPR which are a good resource to have to hand if this situation did arise (13). The ALS algorithm can be followed as with a normothermic casualty, however, the casualty may need warming before return of spontaneous circulation (ROSC) is achieved. To this extent, it is well known that “a casualty is not dead, until they are warm and dead!” These casualties should be warmed to normal body temperature at 37.5°C before a definitive decision is made regarding death. Full recovery can be possible in hypothermic cardiac arrest with ECMO if there was no preceding hypoxia or serious trauma and this has been witnessed in accidental hypothermia of temperatures as low as 14°C (14,15).
How to prevent hypothermia ?
Mountainous expeditions are becoming more accessible and popular and with that, the risk of cold injuries including hypothermia is also climbing. Thorough preparation can prevent hypothermia and thus save lives. Prior to embarking on an expedition, research the environment in which you will be situated. Use this knowledge to prepare a kit list for personal kit, group kit and medical kit. Consider the properties of items you are packing- are they going to be prone to freezing? If so, is there an alternative you could pack instead? Or could you store it in a particular way to ensure it doesn’t freeze? When preparing for an expedition where there may be an increased risk of hypothermia such as in the mountains, consider the following:
- Quantity and quality of clothing and insulation including sleeping equipment
- Quantity and properties of food -what is the estimated calorie requirement for each participant for the expedition, will you still be able to eat your snacks in freezing conditions etc?
- Rewarming kit – hypothermic wrap, storm shelter, bivvi bag, stove, heat packs, spare layers etc
- Shelter options en route
- Group’s knowledge of cold injuries and how to manage them – consider providing everyone with an aide memoire and an educational brief
- Group awareness – consider a buddy system so that team members check in regularly on one another to ensure any suspicious signs are spotted early and dealt with promptly to prevent further clinical deterioration.
Take home messages
- Hypothermia occurs when the rate of heat loss is greater than the rate of heat production
- Hypothermia can be prevented with thoughtful preparation of personal kit, medical kit and team awareness
- Have a low threshold of suspicion of slow, confused or withdrawn members of the team
- Build a hypothermic wrap into kit and ensure it is easily accessible
- Always consider cardiac instability when handling hypothermic patients
- Nobody is dead until they are warm and dead!
References:
- Procter E, Brugger H, Burtscher M. Accidental hypothermia in recreational activities in the mountains: A narrative review. Scand J Med Sci Sports. 2018;28: 2464– 2472. Available at: https://doi.org/10.1111/sms.13294
- J. Enrique Silva. Thermogenic Mechanisms and Their Hormonal Regulation. Physiological Reviews. 2006;86:2,435-464. Available at: https://journals.physiology.org/doi/full/10.1152/physrev.00009.2005
- Duong H, Patel G. Hypothermia. [Updated 2022]. Treasure Island (FL): StatPearls Publishing. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545239/
- Dietrichs E, Håheim B, Kondratiev T, Traasdahl E, et al. Effects of hypothermia and rewarming on cardiovascular autonomic control in vivo. J Appl Physiol. 2018;124:850–859.
- Moore E, Moore H, Kornblith L, et al. Trauma-induced coagulopathy. Nat Rev Dis Primers. 2021;7:30. Available at: https://doi.org/10.1038/s41572-021-00264-3.
- Haman F, Blondin DP. Shivering thermogenesis in humans: Origin, contribution and metabolic requirement. Temperature (Austin). 2017;4(3):217-226. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5605160/
- Haman F, Souza S, Castellani J, Dupuis M, Friedl K, Sullivan-Kwantes W, Kingma B. Human vulnerability and variability in the cold: Establishing individual risks for cold weather injuries. Temperature (Austin). 2022;9(2):158-195. Available at: https://www.tandfonline.com/doi/full/10.1080/23328940.2022.2044740
- Cueni-Villoz N, Devigili A, Delodder F, Cianferoni S, Feihl F, Rossetti A, Eggimann P, Vincent J, Taccone F, Oddo M. Increased blood glucose variability during therapeutic hypothermia and outcome after cardiac arrest. Crit Care Med. 2011;39(10):2225-31.
- Grant I, Cosgrove H, Thomson L, Guly H et al. Kurafid – The British Antarctic Survey Medical Handbook. BASMU: Plymouth: British Antarctic Survey; 2005.
- Pasquier M, Carron P, Rodrigues A, et al. An evaluation of the Swiss staging model for hypothermia using hospital cases and case reports from the literature. Scand J Trauma Resusc Emerg Med. 2019;27:60. Available at: https://doi.org/10.1186/s13049-019-0636-0
- Zafren K. Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia. Emerg Med Clin North Am. 2017;35(2):261-279. Available at: https://www.sciencedirect.com/science/article/abs/pii/S0733862717300032?via%3Dihub
- Dow J, Giesbrecht G, Danzl D, Brugger H, Sagalyn E, Walpoth B, et al. Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update. Wilderness & Environmental Medicine. 2019;30:4:S47-S69.
- Caple A. Casualty Care revision in Mountain Rescue. LAMRT. 2019 (digital edition).
- Štěpán J, Šulda M, Tesařík R, Zmeko D, Kutab B, Schaffelhoferová D, Foral D. Hypothermic Cardiac Arrest Managed Successfully by Changing ECMO Configurations. Journal of Cardiothoracic and Vascular Anaesthesia. 2022;36:12:4413-4419. Available at: https://www.sciencedirect.com/science/article/abs/pii/S1053077022005742
- J. Hilmo et al.“Nobody is dead until warm and dead”: prolonged resuscitation is warranted in arrested hypothermic victims also in remote areas—a retrospective study from northern Norway Resuscitation. 2014. Available at: https://www.sciencedirect.com/science/article/pii/S0300957214005243

Are you interested in learning more about hypothermia and other high altitude conditions?
If so, why not check out our Altitude Medicine Course ? Whilst you’re there, why don’t you take a look at our other courses too?
Leave a Reply
You must belogged in to post a comment.